Iodine, Supplement Reactions, Hormones and More KMUD - Ask Your Herb Doctor - 2016
https://dl.dropboxusercontent.com/u/22195338/kmud_FPS160219_FPS190002fritalk.mp3
HD1 – Andrew Murray
HD2 – Sarah Johannesen Murray RP – Ray Peat
Transcribed by moss, verified by Sheila
HD intro not transcribed
_____________________
HD 1: So brain development, aging and the hormones involved in that gradual decline in good health. So just for people listening to the show, we will be taking calls from 7.30 to the end of the show either related or unrelated to this month’s continuing topic of Nitric Oxide (NO) and wanted to get into a little bit of the subject of Iodine as an opener for the show for people thinking about supplementing with iodine and also open up a little bit about the Zika virus that’s really catching media attention here. I know there’s certain authoritative reasons for it and there are other supposedly conspiracy theories, if you can call them conspiracies, I think some of the merits of conspiracies are worth picking up and exploring. Anyway, if you live in the area, the number here is 1800 568 3723 or 9233911.
HD1: So Dr Peat, I was looking today and I guess what prompted it was hearing advice of people touting a product called nascent iodine and I know that you specialized in thyroid hormone and that iodine is definitely a key component of thyroid hormone. And I think we’ve always been led to believe that there has been adequate supply of iodine in the diet and then they produced iodized salt back in the 50s or 60s, perhaps earlier or not, I’m not too sure, but iodized salt has been around and seafood also contains a lot of iodine in its own right. So when I heard about this product called nascent iodine they were saying that it was essentially not the stable, so stable ionic form and was more available and it’s more readily taken up by the thyroid gland and then I read some other articles about nascent iodine and how reactive it was and I just wanted to feel you out, what you know about the thyroid’s natural need for iodine, whether or not we are deficient and whether or not we need supplementation and if in fact, this is something that actually may not be necessary.
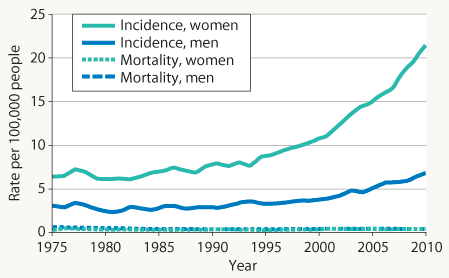
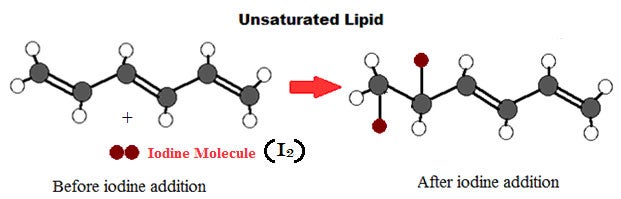
RP: In the 1980s, I was looking into the iodine nutrition question because I saw some women with breast disease who recovered quickly when they took supplements of kelp or thyroid hormone and the safest thing, I think, is to correct the thyroid problem directly rather than counting on big doses of iodine because the large doses over many years, for example, there are about 70 or more publications looking at iodine intake around the world, over a period of decades, and they see that over half a mg or even especially over 1mg of iodine per day over a population is closely connected with increased risk of thyroiditis and thyroid cancer. One of the theories of why that happens is that iodine spontaneously reacts, or in the presence of white blood cells their enzymes can cause iodine to react with fatty acids that are unsaturated. And if you’ve heard about the iodine number to describe the degree of unsaturation of the fats - for example, the food oils that are highly unsaturated have a high iodine number. That means the number of molecules of iodine that will be spontaneously absorbed by a certain quantity of the oil, because the iodine attacks the double bonds in the fats and where they lack hydrogen saturation, the iodine fills in like an analogue to the saturated hydrogen content. So there is this tendency of unsaturated fats to react with iodine and when that happens the body can then interpret that as a signal to the thyroid gland, possibly imitating the thyroid-stimulating hormone (TSH).
HD 1: Really?
HD2: So it doesn’t cause an increase of thyroid hormone?
RP: It can fill the site where TSH should be acting and it can interfere with that, so it can probably go either way, forcing too much activity, or more likely blocking the effect of TSH. The polyunsaturated fats (PUFAs) by themselves interfere with the enzyme which releases thyroid hormone from the glands, so too much of the unsaturated fats with or without iodine will have an anti-thyroid effect. But potentially the iodine reaction could cause overstimulation by TSH or in its place could imitate the action.
HD1: Dr Peat, you mentioned the iodine binding to the double bonds producing this product and in it’s own right that could stimulate an inflammatory thyroiditis and/or a cancer?
RP: Yeah. I think that’s why the high iodine intake around the world statistically associated with greater risk of thyroid cancer and if there really were a product that contained a more reactive form of iodine, that would just mean that it would attack more molecules, but I looked up the sources of that product and one of the products started about 10 years ago. A man in Texas filed a patent that is just completely goofy. If you look at the diagram, it shows things that just can’t happen and so it was filed 10 years ago and I think it still hasn’t been and probably never will be actually approved as a patent. But you can apply for a patent on any goofy idea and then publish the application and impress a lot of people!
HD1: But maybe not bring the product to the market.
HD2: So iodine supplementation is very risky and basically you should get your trace minerals from seafood sources, rather than from isolated iodine supplements and especially not in combination with any kind of vegetable polyunsaturated oils.
RP: Yeah I think that’s true.
HD 1: So, just to quickly wrap up this nascent iodine, I think the reason that it caught my attention was that the media spin on was that it because it didn’t have, any chemistry people hearing this will understand what I’m saying and can go and elaborate it more simply perhaps, but it doesn’t have a stable octet so its outer electron shell isn’t filled. And they were saying that because of this, it was much more suitable in some way to occupying these sites in the thyroid to produce thyroid hormone, but its very reactivity is counterproductive, because surely, if you keep it as unreactive as that in a bottle waiting for to be ingested, wouldn’t it surely react with one of the first things it came into contact with when you ingested it - just to fill its octet and become stable again?
RP: Oh yeah. The whole idea of a “newly born” nascent molecule, when I was in junior high, in high school, the chemistry people talked about nascent oxygen which for a few seconds after it’s formed in a certain way is highly reactive but that’s because the electrons are simply in an excited state, like it had been sitting in the sunlight too long. That’s an electronic excitation which quickly passes as it gives off a little bit of energy but in certain short term situations a few seconds, that kind of excited electron state can make a molecule useful for certain reactions but isn’t something you’d want to put your body through.
HD 1: So, not for in vivo use, but maybe in vitro experimentations, it might have some kind of a use?
HD2: So it’s basically a more dangerous form of iodine that can cause a free radical reaction?
RP: Yeah, that’s what they are talking about but I don’t think it even exists in the product?
HD1: So, Dr Peat, I was looking at some abstracts here that were going to form the show and the first couple caught my attention just because they were based on isoflavones and I know from our studying herbal medicine, soy and isoflavones were all the rage and were touted as being very health beneficial, reducing cholesterol and all this other ridiculously unscientific information that was purported. So from the basis of soy, they mentioned that there was an alcohol soluble fraction that had been shown essentially to basically cause female cancers, that these things were taken up by the thyroid or rather they inhibited the uptake of iodide by the gland and that this increased the oestrodial in females and that this was, I know that we’ve heard about soy and now we definitely are aware of soy being very pro-carcinogenic because it’s an oestrogen mimic. What do you think about this whole industry push that was producing, and probably still is producing, soy infant formula, which is one of the main foods that was generated from it?
RP: I think it has seriously harmed lots of kids by partly the oestrogenic effect. The oil itself has a pro-oestrogen effect, anti-thyroid effect. Apart from those little molecules, the isoflavones, the category of flavones or flavonoids, it’s very similar to the isoflavones, the phenyl group or benzene group is just located slightly closer to the keto oxygen in the isoflavones and that group seems to be the oestrogenic group. The other orientation of the benzene group makes it more likely to be anti-oestrogenic and lots of fruits and vegetables contain the anti-oestrogenic forms of those, but the oestrogen industry as a background, led to a lot of the sales talk about the effects of soy chemicals.
HD1: And of course there is a hugely cultivated GMO products patents owned for its propagation and its use again no doubt another spawned product from big corporations who essentially want to own the product.
HD2: But don’t all legumes have a certain percentage of these isoflavones? [RP: Aha] But just soy is particularly high?
RP: No. I think the main problem with soy besides it basically being inedible; I think the main problem is that it’s almost all from grown in the genetically modified form that takes large amounts of toxic pesticides.
HD2: Which are oestrogenic too, right? RP: Yeah.
HD2: And again, just for the guys out there, I think it is very important to make you aware that guys have oestrogen. It’s not just a female-dominated situation and soy consumption in males has also been positively associated with gynecomastia, which is another side effect if you like of oestrogen activity within males. The very same thing, Dr Peat, isn’t it with alcohol and drinking alcohol excessively can produce that symptom of male breasts that is an oestrogenic type reaction?
RP: When I was a kid, just before the Second World War, we knew some of the very poorest immigrants to California and there was one couple in which the wife got a job but the father could nurse the baby because his oestrogen had become so high from malnutrition and at the end of the Second World War when soldiers got out of the prison camps, lots of them had breasts from the effects of prolonged starvation.
HD1: Are we talking lactation too?
RP: Well, in the case of this man in California, the wife said, “Pa’s milk ain’t got much strength”.
Yeah, they can lactate if they have a baby nursing.
HD: Wow! So there’s enough positive feedback in the physiological mechanism, inherently to produce that?
HD2: So I guess that high oestrogen stimulation raised their prolactin?
RP: Yeah.
HD2: And with the suckling it produced milk?
RP: Yeah.
HD2: Wow, that is just absolutely incredible.
HD1: OK - so again just for people that are listening, it just begs the question again where things like soy and soy products, all we ever hear.... We don’t have a television, we don’t have a TV at all, but we don’t listen to broadcasts from mainstream media. But what I was going to say was that most people have a TV or they listen to a regular radio station, getting the same spin put on things and the same sales pitch and so I just find it hard to believe that for a long time the whole soy thing could exist and it could do what it did - when actually it’s more like a waste product and people really shouldn’t be eating soy because it’s so dangerous in terms of its oestrogenic effects on females and males and those oestrogenic effects are very pro-inflammatory. Dr Peat, you have pointed that out many, many occasions and I am currently on board with that same feeling that the irritation and the inflammation that oestrogen promotes is nothing but a dangerous process in the body.
HD2: And also Dr Peat, how would you compare oestrogen levels with menopausal women and men?
RP: With aging, a man’s oestrogen pretty steadily increases but if he has a heart attack it goes up sharply or if he has a traumatic injury it goes up during the recovery time - but generally there’s a trend upward in men and in women when the ovaries stop cycling and up until about the age of 38–40 there is an actual steady increase in the oestrogen and when the ovaries stop cycling, they stop suddenly producing progesterone but they continue producing a considerable amount of oestrogen until the body can adjust it downward. So there are a few years in the 40s or early 50s usually, when oestrogen is extremely excessive relative to the anti-oestrogen effect of progesterone. But then again after the ovaries have pretty much stopped functioning, the rest of the body, as the progesterone fails, all the other tissues begin, similarly it happens in men, all of a woman’s tissues tend to start increasing their production of oestrogen so that after menopause, the fatter a woman is, the more oestrogen she’s producing because the fat tissue is a good source of it. But any tissue after menopause to the degree that it’s stressed, will begin producing oestrogen.
HD2: So is that about the same level between men and women, after the menopausal period?
RP: Yeah, I think woman tend to be fatter in old age and so they are more likely to have a higher level of oestrogen. But just measuring the blood oestrogen gives a misleading impression because when progesterone is deficient, the oestrogen receptor as well as the aromatase enzyme that makes oestrogen, the receptors binded in cells and there’s no progesterone to destroy the oestrogen receptor so it just stays in the cell and some of the enzymes that are no longer inactivated by progesterone, other enzymes capture circulating oestrogen that should have been excreted, cause it to be deposited in cells still other enzymes shift any oestrogen away from the oestrone form to the oestriol form which is the most active, intense oestrogen. So everything that happens when progesterone is deficient tends to load up various cells all through the body with more and more oestrogenic stimulation, even though, it isn’t being released to be measured in the blood.
HD2: Right, so the blood test could appear that it’s fine but if you have a large amount of fat cells it could be stored in that and other tissues. And what about weight loss for woman who are in the menopause state, to lose that weight do they then poison themselves with that oestrogen as it comes out of the cells?
RP: Just temporarily, but it’s better to get rid of it than have it local because inside the cells because it produces things such as breast cancer, lung cancer, uterine cancer, ovarian cancer, all of the tissues that no longer have enough progesterone are subject to cancer infestation.
HD2: So what about the women that continue to menstruate, like I heard from this lady the other day, that she had this friend who was 70 and was still menstruating?
RP: I talked to a gynaecologist, who was giving his wife progesterone and she was still menstruating at 60. And if you happened to have a very good system for producing progesterone there’s no reason why it should stop at 55.
HD2: So there’s no reason to stop at 55 then, right?
RP: No.
HD2: So basically do you think it would be beneficial that woman to continue to menstruate until the day they die?
RP: I think so.
HD2: Like the flamingos.
RP: Yeah the flamingos have no life limitation according to ordinary mortality curves cause they seem to only die by accidents.
HD2: Or starvation.
HD1: Dr Peat, I wanted to pick up on the point that you mentioned during your last discourse there. I’ve not heard that before: Progesterone destroys the oestrogen receptor? Does anything similarly happen with oestrogen doing the same thing to progesterone receptors or is it just that way around?
RP: Well, oestrogen activates its own receptor in most tissues and it will activate inflammatory things, which tend to turn off the progesterone receptor, if you have excess. Generally, the normal function would be for progesterone to rise as soon as the oestrogen has had its surge and then knock it out. The oestrogen is fine if it is active only for 12-24hrs every month.
HD2: It does its job and then it’s finished.
HD1: But like you said the tissues will carry on producing oestrogen in tissues especially in
obese individuals and menopausal or even postmenopausal women.
HD1: OK, so just another call for all the ladies out there that there really is nothing, and I know it is a personal thing, but nothing wrong with continuing your menstrual cycle as long as you possibly can Progesterone is your friend, oestrogen is your enemy and the only thing really that oestrogen is any good for is the implantation and so we have our first caller, so let’s get this first caller. Caller, where are you from?
Caller: Kansas City. Hi Dr Peat, what do you think is happening if someone experiences digestive cramps and bloating within 30 minutes when using vitamin E orally and which still occurs even when switching to a few different products as well as when using several drops of Progest-E which also contains vitamin it E.
RP: I think it’s the viscous oily quality that is irritating if you are... some people have that reaction, for example, if they try to use it in their armpits where the skin is very sensitive, the highly viscous oil can be very irritating and so I think it should be taken with food so that it doesn’t hit any of the membranes in the concentrated form.
Caller: Do you think it is possible to develop a soy allergy somewhere along the way?
RP: Yeah. Many people do have soy allergies but the oil doesn’t contain any of the proteins that people are allergic to, so I haven’t heard of any documented allergies to the oily soy products such as soy oil.
Caller: OK, do you think it’s possible for that person to have something like 400 IU alpha tocopherol, with 300mg of gamma, delta, beta tocopherol receptors is excessive and possibly be excreted mostly in bile, which is alkaline and possibly irritating to an already irritated intestine which would be the cause of cramps and bloating?
RP: I doubt it because the effect of vitamin E on many cell processes is anti-inflammatory - for example, it inhibits prostaglandin formation similar to aspirin and its range of anti-inflammatory effects.
Caller: OK. That’s great, thank you.
HD1: First caller from Mexico! Welcome to the show. What’s your question?
Caller: Thanks. Hi, if I understood correctly, earlier you were talking about how taking extra iodine can interact with PUFAs to cause problems and I know someone who took a few mgs of extra iodine and she went into some kind of thyroid, hyperthyroid-like crisis state where she couldn’t tolerate any physical exertion. Her muscles were really weak and her pulse was very high and years later she still gets that reaction from thyroid and I was wondering if that’s related to iodine?
RP: Back in the years when many people were in certain regions, for example, in Southern Mexico, Western China, Ohio and Eastern Europe, those areas were very deficient in iodine and they would develop an enlargement of the thyroid gland and then when they ate iodine even a fairly normal amount, suddenly their gland would start forming thyroid hormone and if the goiter was very big they could have serious hyperthyroidism that could last for years but, if the gland was just slightly swollen, it would pass in about two months.
HD1: So that’s a very real sequelae of using iodine in that particular individual that they would have that increased thyroid production that would result in what the caller’s just mentioned?
RP: Yes if they took their iodine in the form of thyroid hormone they could normalize their body functions and be replacing iodine in a limited graded fashion and so they wouldn’t go into those hyperthyroid states and getting the required amount of hormone would cause their pituitary to settle down and let the gland gradually shrink.
HD2: And so that is treatment for goiter, is that you supplement with thyroid hormone?
RP: Yes to treat hyperthyroidism the safest thing is to supplement usually with thyroid hormone.
HD1: OK, and so again just to expand on the very first question to Dr Peat about the nascent iodine - not a good idea and also many other forms of iodine supplementation are not necessary - and if you need iodine and you have any kind of low thyroid actually thyroid hormone is the best way to get bound iodine. And did you have anything else you would like to bring up, Caller?
Caller: Well, thanks for that and I was just wondering if you know if it would be a good idea to do anything specific to try to rectify this problem or if there’s any tips on tolerating thyroid, would avoiding iodine help in a situation like that?
RP: The people who have trouble with the actual thyroid hormone they can be either deficient in magnesium because hypothyroidism makes all of your tissues fail to retain a normal amount of magnesium and then when you supplement it, suddenly you experience an extreme magnesium deficiency in your heart, for example, and your brain, and so taking some magnesium at the same time as the thyroid will help those people. Others, if they are deficient in adrenal or ovarian or gonadal steroids, will suffer stress symptoms when they take thyroid and so using a supplement such as pregnenolone will make them tolerate adapting to the thyroid hormone more easily.
HD2: And what about, Dr Peat, how some people if they supplement with T4 thyroxine, they will have those symptoms like our caller mentioned where their muscles are weak and their heart’s
pounding, and their pulse is high and isn’t that because if they are already low thyroid and they take the T4 then are actually stimulating the adrenalin because they are not converting it?
RP: Yeah. When people have suffered for a long time with a low thyroid they are likely to have extremely high adrenalin and cortisol levels and that causes them to turn T4 into reverse T3 blocking the actual active T3 hormone and then if they accumulate more and more T4 that will interfere competitively with the little bit of T3 that they do have, so they can exaggerate the state of their hypothyroidism if they’re in that extreme stressed state.
HD1: Would you say that T4 perhaps is maybe only 10% as active as the active T3 hormone?
RP: It really varies. In the 1940s, when they first synthesized it, they tested it on male medical students and it was exactly as effective as Armour natural thyroid and that’s because young men, 20-22 years old, have very good livers that can perfectly convert it, but even at the same age women are more likely to have problems with plain thyroxine.
HD1: So when you talk about T4 being weakly active, how do you interpret that or how do you see T3 versus T4 in terms of orchestrating metabolic events?
RP: Well the standard textbook idea is that T3 is 4 times more powerful than T4 but really if your liver is good you can get 100% of the benefit out of T4 and if you are a woman under stress with high oestrogen your liver isn’t going to convert any of it to the right active hormone, and the more you take – I’ve known of one woman who was hospitalized and got more and more hypothyroid the higher they raised her thyroxine dose - and as soon as they gave her T3 she came right out of the myxedema coma, but I have seen people in less extreme states who got more and more depressed or psychotic or whatever when they increased their thyroxine dose.
HD2: I have one more question for the caller. Do you know if this lady you’re speaking about was taking a T3/T4 combination supplement or were they taking just T4 or just T3? Are you aware of that?
Caller: Yeah, well, originally she was taking an Armour supplement and when she took the supplemental iodine that caused the problem and since then she has tried different T4/T3 combo products, as well as a couple of different, pure T3 supplements. So I think it’s something to do with this adrenalin or sensitivity to adrenalin that Dr Peat was talking about, where if I understand him correctly, the thyroid sensitizes the tissues to the already high, the already existing adrenalin.
HD2: But that should only last a couple of days and then it should balance out.
RP: Well, sometimes it lasts for a couple of weeks. If you’re really extreme, you have to use little bits of supplements and be very careful about your intake of protein, sugar, calcium, everything that is counter to the stress.
Caller: So when you are in a situation like that she was using very small specks of T3, under 1 mcg sometimes. Is the thing to do to hold that very low dose for a couple of weeks, then increase it in very, very small increments as the adrenalin hopefully comes down?
RP: Yeah. I’ve known people for a week or two who would stay with 1mcg doses of T3, but you have to make sure your whole diet is very good, having hormone tests, and a vitamin D blood test is helpful because magnesium and calcium work together and vitamin D regulates them.
HD2: Yeah and making sure that she’s getting plenty of carbohydrates like in the form of fruit juices because that’s like Dr Peat is saying - making sure nutritionally that she is getting at least 75g of protein and - I don’t know the weight and nutritional needs –but at least 150 grams of more sugars and good fats.
Caller: OK, thanks very much.
HD2: OK – I think have another caller. Caller, where are you from? Caller: Hi, I’m calling from New York.
HD1: Welcome to the show what is your question?
Caller: I have a question for Dr Peat about Buteyko breathing and heart rate. Dr Buteyko noted that as you progress with retaining more and more Co2 with the Buteyko breathing, then the heart rate will decrease and I wondered what you thought about that. I’ve noticed that in my own practice that it does go down but the temperature is still good and I wondered if the metabolism is still good when that happens or what you think about it?
RP: Yeah, there have been experiments with animals increasing their Co2 and watching what happens to the heart and blood vessels and Co2 relaxes the blood vessels so it decreases peripheral resistance and that makes the heart able to pump more blood more easily with less work. So it usually means a bigger stroke volume.
HD2: So the decreased heart rate is a good thing.
Caller: OK, so even though it’s a lower heart rate you think that you can still get the same benefits as you would if your weren’t restricting your breathing but... I know you recommend a high heart rate typically for people that aren’t practicing that kind of breath control?
RP: Yeah, but most people are running on adrenalin and I’ve known people, one woman who had a 180 pulse steadily for years, another person had been around a 130 resting pulse for a long time, and both of these people within two weeks got down to a normal under a 100 pulse rate when they supplemented thyroid. And one of the things the thyroid is doing is increasing your Co2 and decreasing the lactic acid and the inflammation so that your capillaries open up, you have less peripheral resistance, so your heart doesn’t have to work so frantically.
Caller: OK, well thank you very much.
HD1: OK, so it’s always good to get people all over the States and so we’ve had Mexico so far, New York, Midwest and so let’s keep it up. I wanted to ask you - we haven’t actually got very far through all the questions I wanted to ask you at this point - and this is good news because people have been calling and I may have to carry over this topic to next month if you are available. I saw the article there which again highlights the oestrogenic problem, that the benign and malignant thyroid nodules are far more common in females than males and no doubt a consequence of oestradiol, so given that the mainstream lie is that oestrogen is good for you and healthy, what can be done you think simply to offset the oestrogen, and I now know we’ve mentioned progesterone, which is probably the first that springs into my mind, but in terms of reducing a female’s oestrogenic burden?
RP: There were some studies of slices of thyroid gland in vitro and they found that added oestrogen caused the cells to keep synthesizing hormone and to keep growing, but failed to secrete any of the hormone. When they added progesterone it began secreting the hormone. And up until the last few decades women, rather than just having nodules in their thyroid, they were the ones most susceptible to growing a very large goiter that sometimes was as big as a cantaloupe - and the nodules are basically the same process of oestrogen activating the cell division and synthesis of colloid - the material that the hormone later will be made from - and desensitizing the cells to the hormone secreting effect of TSH and progesterone by antagonizing oestrogen will reverse those processes, but when you get the cells multiplying and making the protein you will get at least a nodule, maybe if it continues steadily, the whole gland will get bigger and bigger.
HD1: We actually do have another caller - so let’s hold that thought and take this next caller. Caller, where are you from?
Caller: I’m from right here in town. I was curious to know - I heard you talking about the vitamin D and the thyroid and the magnesium. I was just wondering if that would have anything to do with what’s called “restless leg syndrome”?
HD2: Yes, that’s a magnesium deficiency. Dr Peat, how would you explain restless leg syndrome?
RP: There has been quite a lot of research about it and, for example, they noticed that people taking SSRI antidepressants tended to have episodes of restless legs and so they saw that Nitric Oxide (NO) and serotonin were involved in producing it. Those are produced largely from the intestine. The most intense problem of both serotonin and NO production is from an irritated intestine and hypothyroid people overproduce both NO and serotonin typically and have sluggish digestive systems and often have a tendency to generalized inflammation. And the serotonin seems to be specifically what pushes those motor nerves that cause the leg jumpiness.
HD1: Does that help you out or explain things to you, Caller?
Caller: Yeah. So it’s not an adrenalin thing that makes the legs jump - it’s serotonin?
RP: All of the inflammatory stress things tend to go together.
HD2: So, would you recommend aspirin for restless leg syndrome?
RP: Yep, pregnenolone, aspirin, and avoiding irritating foods, especially legumes and raw green salads. Those are very irritating.
HD2: Those are things that increase the bowel production of serotonin.
RP: Yeah.
HD2: Beans and raw vegetables?
Caller: That’s interesting; cause we just switched to trying to eat better and we had gone to eating more of both of those!
HD2: Had you noticed that your restless leg syndrome had increased?
Caller: It’s a female, and my partner, who experiences this and is becoming very extreme and so that may very well be just from the diet, huh? And she has a vitamin D deficiency and she was told to take vitamin d and magnesium.
HD2: Do you know what her vitamin D level was and how much she is taking? Caller: I don't know exactly in measurement, but it was very low.
HD1: Well, most drop forms of vitamin D now are 2,000 IU a drop and if she has low vitamin D it’s probably below 20, maybe right around 20, which is very low, and they’ve raised the reference limit now for vitamin D to about 45 - so if you are supplementing with a 2,000 IU per day drop product, she should really be loading up with 6-8 drops a day for about 4 or 5 days and then getting around 4,000 to 6,000 IU and then re-measuring her vitamin D levels.
HD2: After about 2 months.
HD1: So, Dr Peat said that bowel irritation/inflammation increases serotonin production and that serotonin production with NO which we have another question for Dr Peat about NO. Both those two compounds there can be predisposing someone to restless leg syndrome. Anyway, thanks for your call.
HD1: So, Dr Peat I saw, today just in fact - and I was thinking about it myself and started looking at a couple of websites that do blood testing etc. and I couldn’t see any NO blood testing tests done - but I did see salivary tests for – they were salivary nitrite strips to assess the potential NO production in the body. I know it will be formed from nitrate or nitrite. This is the funny thing, this site actually was letting you know how you could increase NO more by eating various foods which I wanted to question you about also - so I know some of the greens here that are promoting the NO production are some of the things that we are actually promoting as being beneficial but there’s obviously a reason for that. So how do you feel about testing your salivary nitrate/nitrite level and how predictive or pre-emptive that would be of NO production systemically?
RP: A recent article just a couple of weeks ago came out suggesting measuring the NO or its products in the body as a way of diagnosing hypothyroidism because they are so closely connected, but I would guess that the urine might be better than the saliva because for other hormone testing, for example, just thinking of food or being anxious or whatever can really change the composition of your saliva.
HD1: OK, so because that changes so quickly, your saying, that it is more relative to test something that’s there and it’s stored and probably more representative of a couple of hours of physiology?
RP: Yeah. I think that the urine will give you a good picture of your level of stress.
HD2: You wouldn’t want to test it after eating spinach either with your saliva.
HD1: Here’s the other thing – this was my other question - this website was touting NO as being beneficial and actually spinach was a very good producer of nitrate, and how spinach will increase your NO - and they were touting that - and I know and I want to ask you here just to be realistic and be real for folks - I know we mentioned greens, purporting greens, and boiled greens and drinking the juice as very beneficial and I know that you do say kale can have a thyroid suppressant effect - so not to use to much kale - but spinach I think has been one of those greens that has been portrayed as being relatively healthy - so what do you think about spinach?
RP: If they are organically grown without intense nitrate fertilization and if it’s well cooked, I think spinach is good food.
HD1: Let’s take this next caller. Caller, where are you from?
HD1: You’re on the air, where are you calling from?
Caller: Hi, I’m from Shelter Cove. My question is for my daughter actually. She wants to take testosterone and I’m wondering what Dr Peat’s take is on it and if he has any experience on that and how she can keep herself healthy?
HD1: How old is she and what is the indication for taking the testosterone? Caller: Well, she is transgender and wants to be more male and she is 16.
RP: Wanting to masculinize?
Caller: Yes.
RP: I think that’s safe but it should be backed up with pregnenonlone and some progesterone to keep things in balance because the tendency is, if you are under stress of any sort, for the testosterone to turn to oestrogen and the pregnenolone and progesterone will limit that conversion.
Caller: OK.
HD1: Do you have access to those? Both of those can be obtained, so progesterone and pregnenolone, typically for a female anyway they would normally be producing them and I don't know the exact details of the case and how the transgender nature of this subject is either affected her adversely or positively and so in terms of their exposure to their own natural progesterone being female and/or supplementing with pregnenolone, then that would offset the potentially negative effects that may occur with using testosterone in a female.
HD2: Cause it could convert to oestrogen and become dangerously out of balance. RP: And watching thyroid function.
Caller: OK. Thanks for your help.
HD1: I don't even know if we have enough time to ask another question without running out of time, but I’ll try here. And I think we will definitely open this up for the next month if you are available cause we hardly got any questions asked cause we had so many callers and that’s a good thing. I wanted to ask you again with the female issue and oestrogen and inflammation and cancers etc., pretty obvious as definite realities here. In terms of the effects of iodine uptake by thyroid cells, and the inhibitory effects oestrogen has on that, in a female, again would you be just typically wanting to lower oestrogen burden by offsetting that with progesterone and pregnenolone and/or thyroid?
RP: Yeah, thyroid and good adequate nutrition. All the vitamins and minerals are involved in controlling and keeping oestrogen under the safe limit. And when you inhibit the formation of thyroid hormone, either with an iodine deficiency or an oestrogen excess, the TSH fails to make the thyroxin and T3 and so it keeps stimulating not only the thyroid gland, making it grow and get bigger or nodules to form, but it has a related effect on every tissue to some extent - especially the ovaries. Polycystic ovarian syndrome (PCOS) is associated with low thyroid and especially high TSH. TSH drives inflammation so that the so- called autoimmune conditions associated with high oestrogen - women are far more susceptible to all types of autoimmune diseases than males - and that's largely because of the high TSH exposure driving things like tumor necrosis factor and the various cytokines, and interleukins and prostaglandins that are activated.
HD1: Excellent. I don’t want to cut you short Dr Peat and I really appreciate your knowledge, as do I know all the people that are tuned in and taken the time to listen and to call from all over. A really good show from people all over the country and I really appreciate people calling. Thanks very much, Dr Peat.
www.raypeat.com
_______________________
https://dl.dropboxusercontent.com/u/22195338/kmud_FPS160219_FPS190002fritalk.mp3
HD1 – Andrew Murray
HD2 – Sarah Johannesen Murray RP – Ray Peat
Transcribed by moss, verified by Sheila
HD intro not transcribed
_____________________
HD 1: So brain development, aging and the hormones involved in that gradual decline in good health. So just for people listening to the show, we will be taking calls from 7.30 to the end of the show either related or unrelated to this month’s continuing topic of Nitric Oxide (NO) and wanted to get into a little bit of the subject of Iodine as an opener for the show for people thinking about supplementing with iodine and also open up a little bit about the Zika virus that’s really catching media attention here. I know there’s certain authoritative reasons for it and there are other supposedly conspiracy theories, if you can call them conspiracies, I think some of the merits of conspiracies are worth picking up and exploring. Anyway, if you live in the area, the number here is 1800 568 3723 or 9233911.
HD1: So Dr Peat, I was looking today and I guess what prompted it was hearing advice of people touting a product called nascent iodine and I know that you specialized in thyroid hormone and that iodine is definitely a key component of thyroid hormone. And I think we’ve always been led to believe that there has been adequate supply of iodine in the diet and then they produced iodized salt back in the 50s or 60s, perhaps earlier or not, I’m not too sure, but iodized salt has been around and seafood also contains a lot of iodine in its own right. So when I heard about this product called nascent iodine they were saying that it was essentially not the stable, so stable ionic form and was more available and it’s more readily taken up by the thyroid gland and then I read some other articles about nascent iodine and how reactive it was and I just wanted to feel you out, what you know about the thyroid’s natural need for iodine, whether or not we are deficient and whether or not we need supplementation and if in fact, this is something that actually may not be necessary.
RP: In the 1980s, I was looking into the iodine nutrition question because I saw some women with breast disease who recovered quickly when they took supplements of kelp or thyroid hormone and the safest thing, I think, is to correct the thyroid problem directly rather than counting on big doses of iodine because the large doses over many years, for example, there are about 70 or more publications looking at iodine intake around the world, over a period of decades, and they see that over half a mg or even especially over 1mg of iodine per day over a population is closely connected with increased risk of thyroiditis and thyroid cancer. One of the theories of why that happens is that iodine spontaneously reacts, or in the presence of white blood cells their enzymes can cause iodine to react with fatty acids that are unsaturated. And if you’ve heard about the iodine number to describe the degree of unsaturation of the fats - for example, the food oils that are highly unsaturated have a high iodine number. That means the number of molecules of iodine that will be spontaneously absorbed by a certain quantity of the oil, because the iodine attacks the double bonds in the fats and where they lack hydrogen saturation, the iodine fills in like an analogue to the saturated hydrogen content. So there is this tendency of unsaturated fats to react with iodine and when that happens the body can then interpret that as a signal to the thyroid gland, possibly imitating the thyroid-stimulating hormone (TSH).
HD 1: Really?
HD2: So it doesn’t cause an increase of thyroid hormone?
RP: It can fill the site where TSH should be acting and it can interfere with that, so it can probably go either way, forcing too much activity, or more likely blocking the effect of TSH. The polyunsaturated fats (PUFAs) by themselves interfere with the enzyme which releases thyroid hormone from the glands, so too much of the unsaturated fats with or without iodine will have an anti-thyroid effect. But potentially the iodine reaction could cause overstimulation by TSH or in its place could imitate the action.
HD1: Dr Peat, you mentioned the iodine binding to the double bonds producing this product and in it’s own right that could stimulate an inflammatory thyroiditis and/or a cancer?
RP: Yeah. I think that’s why the high iodine intake around the world statistically associated with greater risk of thyroid cancer and if there really were a product that contained a more reactive form of iodine, that would just mean that it would attack more molecules, but I looked up the sources of that product and one of the products started about 10 years ago. A man in Texas filed a patent that is just completely goofy. If you look at the diagram, it shows things that just can’t happen and so it was filed 10 years ago and I think it still hasn’t been and probably never will be actually approved as a patent. But you can apply for a patent on any goofy idea and then publish the application and impress a lot of people!
HD1: But maybe not bring the product to the market.
HD2: So iodine supplementation is very risky and basically you should get your trace minerals from seafood sources, rather than from isolated iodine supplements and especially not in combination with any kind of vegetable polyunsaturated oils.
RP: Yeah I think that’s true.
HD 1: So, just to quickly wrap up this nascent iodine, I think the reason that it caught my attention was that the media spin on was that it because it didn’t have, any chemistry people hearing this will understand what I’m saying and can go and elaborate it more simply perhaps, but it doesn’t have a stable octet so its outer electron shell isn’t filled. And they were saying that because of this, it was much more suitable in some way to occupying these sites in the thyroid to produce thyroid hormone, but its very reactivity is counterproductive, because surely, if you keep it as unreactive as that in a bottle waiting for to be ingested, wouldn’t it surely react with one of the first things it came into contact with when you ingested it - just to fill its octet and become stable again?
RP: Oh yeah. The whole idea of a “newly born” nascent molecule, when I was in junior high, in high school, the chemistry people talked about nascent oxygen which for a few seconds after it’s formed in a certain way is highly reactive but that’s because the electrons are simply in an excited state, like it had been sitting in the sunlight too long. That’s an electronic excitation which quickly passes as it gives off a little bit of energy but in certain short term situations a few seconds, that kind of excited electron state can make a molecule useful for certain reactions but isn’t something you’d want to put your body through.
HD 1: So, not for in vivo use, but maybe in vitro experimentations, it might have some kind of a use?
HD2: So it’s basically a more dangerous form of iodine that can cause a free radical reaction?
RP: Yeah, that’s what they are talking about but I don’t think it even exists in the product?
HD1: So, Dr Peat, I was looking at some abstracts here that were going to form the show and the first couple caught my attention just because they were based on isoflavones and I know from our studying herbal medicine, soy and isoflavones were all the rage and were touted as being very health beneficial, reducing cholesterol and all this other ridiculously unscientific information that was purported. So from the basis of soy, they mentioned that there was an alcohol soluble fraction that had been shown essentially to basically cause female cancers, that these things were taken up by the thyroid or rather they inhibited the uptake of iodide by the gland and that this increased the oestrodial in females and that this was, I know that we’ve heard about soy and now we definitely are aware of soy being very pro-carcinogenic because it’s an oestrogen mimic. What do you think about this whole industry push that was producing, and probably still is producing, soy infant formula, which is one of the main foods that was generated from it?
RP: I think it has seriously harmed lots of kids by partly the oestrogenic effect. The oil itself has a pro-oestrogen effect, anti-thyroid effect. Apart from those little molecules, the isoflavones, the category of flavones or flavonoids, it’s very similar to the isoflavones, the phenyl group or benzene group is just located slightly closer to the keto oxygen in the isoflavones and that group seems to be the oestrogenic group. The other orientation of the benzene group makes it more likely to be anti-oestrogenic and lots of fruits and vegetables contain the anti-oestrogenic forms of those, but the oestrogen industry as a background, led to a lot of the sales talk about the effects of soy chemicals.
HD1: And of course there is a hugely cultivated GMO products patents owned for its propagation and its use again no doubt another spawned product from big corporations who essentially want to own the product.
HD2: But don’t all legumes have a certain percentage of these isoflavones? [RP: Aha] But just soy is particularly high?
RP: No. I think the main problem with soy besides it basically being inedible; I think the main problem is that it’s almost all from grown in the genetically modified form that takes large amounts of toxic pesticides.
HD2: Which are oestrogenic too, right? RP: Yeah.
HD2: And again, just for the guys out there, I think it is very important to make you aware that guys have oestrogen. It’s not just a female-dominated situation and soy consumption in males has also been positively associated with gynecomastia, which is another side effect if you like of oestrogen activity within males. The very same thing, Dr Peat, isn’t it with alcohol and drinking alcohol excessively can produce that symptom of male breasts that is an oestrogenic type reaction?
RP: When I was a kid, just before the Second World War, we knew some of the very poorest immigrants to California and there was one couple in which the wife got a job but the father could nurse the baby because his oestrogen had become so high from malnutrition and at the end of the Second World War when soldiers got out of the prison camps, lots of them had breasts from the effects of prolonged starvation.
HD1: Are we talking lactation too?
RP: Well, in the case of this man in California, the wife said, “Pa’s milk ain’t got much strength”.
Yeah, they can lactate if they have a baby nursing.
HD: Wow! So there’s enough positive feedback in the physiological mechanism, inherently to produce that?
HD2: So I guess that high oestrogen stimulation raised their prolactin?
RP: Yeah.
HD2: And with the suckling it produced milk?
RP: Yeah.
HD2: Wow, that is just absolutely incredible.
HD1: OK - so again just for people that are listening, it just begs the question again where things like soy and soy products, all we ever hear.... We don’t have a television, we don’t have a TV at all, but we don’t listen to broadcasts from mainstream media. But what I was going to say was that most people have a TV or they listen to a regular radio station, getting the same spin put on things and the same sales pitch and so I just find it hard to believe that for a long time the whole soy thing could exist and it could do what it did - when actually it’s more like a waste product and people really shouldn’t be eating soy because it’s so dangerous in terms of its oestrogenic effects on females and males and those oestrogenic effects are very pro-inflammatory. Dr Peat, you have pointed that out many, many occasions and I am currently on board with that same feeling that the irritation and the inflammation that oestrogen promotes is nothing but a dangerous process in the body.
HD2: And also Dr Peat, how would you compare oestrogen levels with menopausal women and men?
RP: With aging, a man’s oestrogen pretty steadily increases but if he has a heart attack it goes up sharply or if he has a traumatic injury it goes up during the recovery time - but generally there’s a trend upward in men and in women when the ovaries stop cycling and up until about the age of 38–40 there is an actual steady increase in the oestrogen and when the ovaries stop cycling, they stop suddenly producing progesterone but they continue producing a considerable amount of oestrogen until the body can adjust it downward. So there are a few years in the 40s or early 50s usually, when oestrogen is extremely excessive relative to the anti-oestrogen effect of progesterone. But then again after the ovaries have pretty much stopped functioning, the rest of the body, as the progesterone fails, all the other tissues begin, similarly it happens in men, all of a woman’s tissues tend to start increasing their production of oestrogen so that after menopause, the fatter a woman is, the more oestrogen she’s producing because the fat tissue is a good source of it. But any tissue after menopause to the degree that it’s stressed, will begin producing oestrogen.
HD2: So is that about the same level between men and women, after the menopausal period?
RP: Yeah, I think woman tend to be fatter in old age and so they are more likely to have a higher level of oestrogen. But just measuring the blood oestrogen gives a misleading impression because when progesterone is deficient, the oestrogen receptor as well as the aromatase enzyme that makes oestrogen, the receptors binded in cells and there’s no progesterone to destroy the oestrogen receptor so it just stays in the cell and some of the enzymes that are no longer inactivated by progesterone, other enzymes capture circulating oestrogen that should have been excreted, cause it to be deposited in cells still other enzymes shift any oestrogen away from the oestrone form to the oestriol form which is the most active, intense oestrogen. So everything that happens when progesterone is deficient tends to load up various cells all through the body with more and more oestrogenic stimulation, even though, it isn’t being released to be measured in the blood.
HD2: Right, so the blood test could appear that it’s fine but if you have a large amount of fat cells it could be stored in that and other tissues. And what about weight loss for woman who are in the menopause state, to lose that weight do they then poison themselves with that oestrogen as it comes out of the cells?
RP: Just temporarily, but it’s better to get rid of it than have it local because inside the cells because it produces things such as breast cancer, lung cancer, uterine cancer, ovarian cancer, all of the tissues that no longer have enough progesterone are subject to cancer infestation.
HD2: So what about the women that continue to menstruate, like I heard from this lady the other day, that she had this friend who was 70 and was still menstruating?
RP: I talked to a gynaecologist, who was giving his wife progesterone and she was still menstruating at 60. And if you happened to have a very good system for producing progesterone there’s no reason why it should stop at 55.
HD2: So there’s no reason to stop at 55 then, right?
RP: No.
HD2: So basically do you think it would be beneficial that woman to continue to menstruate until the day they die?
RP: I think so.
HD2: Like the flamingos.
RP: Yeah the flamingos have no life limitation according to ordinary mortality curves cause they seem to only die by accidents.
HD2: Or starvation.
HD1: Dr Peat, I wanted to pick up on the point that you mentioned during your last discourse there. I’ve not heard that before: Progesterone destroys the oestrogen receptor? Does anything similarly happen with oestrogen doing the same thing to progesterone receptors or is it just that way around?
RP: Well, oestrogen activates its own receptor in most tissues and it will activate inflammatory things, which tend to turn off the progesterone receptor, if you have excess. Generally, the normal function would be for progesterone to rise as soon as the oestrogen has had its surge and then knock it out. The oestrogen is fine if it is active only for 12-24hrs every month.
HD2: It does its job and then it’s finished.
HD1: But like you said the tissues will carry on producing oestrogen in tissues especially in
obese individuals and menopausal or even postmenopausal women.
HD1: OK, so just another call for all the ladies out there that there really is nothing, and I know it is a personal thing, but nothing wrong with continuing your menstrual cycle as long as you possibly can Progesterone is your friend, oestrogen is your enemy and the only thing really that oestrogen is any good for is the implantation and so we have our first caller, so let’s get this first caller. Caller, where are you from?
Caller: Kansas City. Hi Dr Peat, what do you think is happening if someone experiences digestive cramps and bloating within 30 minutes when using vitamin E orally and which still occurs even when switching to a few different products as well as when using several drops of Progest-E which also contains vitamin it E.
RP: I think it’s the viscous oily quality that is irritating if you are... some people have that reaction, for example, if they try to use it in their armpits where the skin is very sensitive, the highly viscous oil can be very irritating and so I think it should be taken with food so that it doesn’t hit any of the membranes in the concentrated form.
Caller: Do you think it is possible to develop a soy allergy somewhere along the way?
RP: Yeah. Many people do have soy allergies but the oil doesn’t contain any of the proteins that people are allergic to, so I haven’t heard of any documented allergies to the oily soy products such as soy oil.
Caller: OK, do you think it’s possible for that person to have something like 400 IU alpha tocopherol, with 300mg of gamma, delta, beta tocopherol receptors is excessive and possibly be excreted mostly in bile, which is alkaline and possibly irritating to an already irritated intestine which would be the cause of cramps and bloating?
RP: I doubt it because the effect of vitamin E on many cell processes is anti-inflammatory - for example, it inhibits prostaglandin formation similar to aspirin and its range of anti-inflammatory effects.
Caller: OK. That’s great, thank you.
HD1: First caller from Mexico! Welcome to the show. What’s your question?
Caller: Thanks. Hi, if I understood correctly, earlier you were talking about how taking extra iodine can interact with PUFAs to cause problems and I know someone who took a few mgs of extra iodine and she went into some kind of thyroid, hyperthyroid-like crisis state where she couldn’t tolerate any physical exertion. Her muscles were really weak and her pulse was very high and years later she still gets that reaction from thyroid and I was wondering if that’s related to iodine?
RP: Back in the years when many people were in certain regions, for example, in Southern Mexico, Western China, Ohio and Eastern Europe, those areas were very deficient in iodine and they would develop an enlargement of the thyroid gland and then when they ate iodine even a fairly normal amount, suddenly their gland would start forming thyroid hormone and if the goiter was very big they could have serious hyperthyroidism that could last for years but, if the gland was just slightly swollen, it would pass in about two months.
HD1: So that’s a very real sequelae of using iodine in that particular individual that they would have that increased thyroid production that would result in what the caller’s just mentioned?
RP: Yes if they took their iodine in the form of thyroid hormone they could normalize their body functions and be replacing iodine in a limited graded fashion and so they wouldn’t go into those hyperthyroid states and getting the required amount of hormone would cause their pituitary to settle down and let the gland gradually shrink.
HD2: And so that is treatment for goiter, is that you supplement with thyroid hormone?
RP: Yes to treat hyperthyroidism the safest thing is to supplement usually with thyroid hormone.
HD1: OK, and so again just to expand on the very first question to Dr Peat about the nascent iodine - not a good idea and also many other forms of iodine supplementation are not necessary - and if you need iodine and you have any kind of low thyroid actually thyroid hormone is the best way to get bound iodine. And did you have anything else you would like to bring up, Caller?
Caller: Well, thanks for that and I was just wondering if you know if it would be a good idea to do anything specific to try to rectify this problem or if there’s any tips on tolerating thyroid, would avoiding iodine help in a situation like that?
RP: The people who have trouble with the actual thyroid hormone they can be either deficient in magnesium because hypothyroidism makes all of your tissues fail to retain a normal amount of magnesium and then when you supplement it, suddenly you experience an extreme magnesium deficiency in your heart, for example, and your brain, and so taking some magnesium at the same time as the thyroid will help those people. Others, if they are deficient in adrenal or ovarian or gonadal steroids, will suffer stress symptoms when they take thyroid and so using a supplement such as pregnenolone will make them tolerate adapting to the thyroid hormone more easily.
HD2: And what about, Dr Peat, how some people if they supplement with T4 thyroxine, they will have those symptoms like our caller mentioned where their muscles are weak and their heart’s
pounding, and their pulse is high and isn’t that because if they are already low thyroid and they take the T4 then are actually stimulating the adrenalin because they are not converting it?
RP: Yeah. When people have suffered for a long time with a low thyroid they are likely to have extremely high adrenalin and cortisol levels and that causes them to turn T4 into reverse T3 blocking the actual active T3 hormone and then if they accumulate more and more T4 that will interfere competitively with the little bit of T3 that they do have, so they can exaggerate the state of their hypothyroidism if they’re in that extreme stressed state.
HD1: Would you say that T4 perhaps is maybe only 10% as active as the active T3 hormone?
RP: It really varies. In the 1940s, when they first synthesized it, they tested it on male medical students and it was exactly as effective as Armour natural thyroid and that’s because young men, 20-22 years old, have very good livers that can perfectly convert it, but even at the same age women are more likely to have problems with plain thyroxine.
HD1: So when you talk about T4 being weakly active, how do you interpret that or how do you see T3 versus T4 in terms of orchestrating metabolic events?
RP: Well the standard textbook idea is that T3 is 4 times more powerful than T4 but really if your liver is good you can get 100% of the benefit out of T4 and if you are a woman under stress with high oestrogen your liver isn’t going to convert any of it to the right active hormone, and the more you take – I’ve known of one woman who was hospitalized and got more and more hypothyroid the higher they raised her thyroxine dose - and as soon as they gave her T3 she came right out of the myxedema coma, but I have seen people in less extreme states who got more and more depressed or psychotic or whatever when they increased their thyroxine dose.
HD2: I have one more question for the caller. Do you know if this lady you’re speaking about was taking a T3/T4 combination supplement or were they taking just T4 or just T3? Are you aware of that?
Caller: Yeah, well, originally she was taking an Armour supplement and when she took the supplemental iodine that caused the problem and since then she has tried different T4/T3 combo products, as well as a couple of different, pure T3 supplements. So I think it’s something to do with this adrenalin or sensitivity to adrenalin that Dr Peat was talking about, where if I understand him correctly, the thyroid sensitizes the tissues to the already high, the already existing adrenalin.
HD2: But that should only last a couple of days and then it should balance out.
RP: Well, sometimes it lasts for a couple of weeks. If you’re really extreme, you have to use little bits of supplements and be very careful about your intake of protein, sugar, calcium, everything that is counter to the stress.
Caller: So when you are in a situation like that she was using very small specks of T3, under 1 mcg sometimes. Is the thing to do to hold that very low dose for a couple of weeks, then increase it in very, very small increments as the adrenalin hopefully comes down?
RP: Yeah. I’ve known people for a week or two who would stay with 1mcg doses of T3, but you have to make sure your whole diet is very good, having hormone tests, and a vitamin D blood test is helpful because magnesium and calcium work together and vitamin D regulates them.
HD2: Yeah and making sure that she’s getting plenty of carbohydrates like in the form of fruit juices because that’s like Dr Peat is saying - making sure nutritionally that she is getting at least 75g of protein and - I don’t know the weight and nutritional needs –but at least 150 grams of more sugars and good fats.
Caller: OK, thanks very much.
HD2: OK – I think have another caller. Caller, where are you from? Caller: Hi, I’m calling from New York.
HD1: Welcome to the show what is your question?
Caller: I have a question for Dr Peat about Buteyko breathing and heart rate. Dr Buteyko noted that as you progress with retaining more and more Co2 with the Buteyko breathing, then the heart rate will decrease and I wondered what you thought about that. I’ve noticed that in my own practice that it does go down but the temperature is still good and I wondered if the metabolism is still good when that happens or what you think about it?
RP: Yeah, there have been experiments with animals increasing their Co2 and watching what happens to the heart and blood vessels and Co2 relaxes the blood vessels so it decreases peripheral resistance and that makes the heart able to pump more blood more easily with less work. So it usually means a bigger stroke volume.
HD2: So the decreased heart rate is a good thing.
Caller: OK, so even though it’s a lower heart rate you think that you can still get the same benefits as you would if your weren’t restricting your breathing but... I know you recommend a high heart rate typically for people that aren’t practicing that kind of breath control?
RP: Yeah, but most people are running on adrenalin and I’ve known people, one woman who had a 180 pulse steadily for years, another person had been around a 130 resting pulse for a long time, and both of these people within two weeks got down to a normal under a 100 pulse rate when they supplemented thyroid. And one of the things the thyroid is doing is increasing your Co2 and decreasing the lactic acid and the inflammation so that your capillaries open up, you have less peripheral resistance, so your heart doesn’t have to work so frantically.
Caller: OK, well thank you very much.
HD1: OK, so it’s always good to get people all over the States and so we’ve had Mexico so far, New York, Midwest and so let’s keep it up. I wanted to ask you - we haven’t actually got very far through all the questions I wanted to ask you at this point - and this is good news because people have been calling and I may have to carry over this topic to next month if you are available. I saw the article there which again highlights the oestrogenic problem, that the benign and malignant thyroid nodules are far more common in females than males and no doubt a consequence of oestradiol, so given that the mainstream lie is that oestrogen is good for you and healthy, what can be done you think simply to offset the oestrogen, and I now know we’ve mentioned progesterone, which is probably the first that springs into my mind, but in terms of reducing a female’s oestrogenic burden?
RP: There were some studies of slices of thyroid gland in vitro and they found that added oestrogen caused the cells to keep synthesizing hormone and to keep growing, but failed to secrete any of the hormone. When they added progesterone it began secreting the hormone. And up until the last few decades women, rather than just having nodules in their thyroid, they were the ones most susceptible to growing a very large goiter that sometimes was as big as a cantaloupe - and the nodules are basically the same process of oestrogen activating the cell division and synthesis of colloid - the material that the hormone later will be made from - and desensitizing the cells to the hormone secreting effect of TSH and progesterone by antagonizing oestrogen will reverse those processes, but when you get the cells multiplying and making the protein you will get at least a nodule, maybe if it continues steadily, the whole gland will get bigger and bigger.
HD1: We actually do have another caller - so let’s hold that thought and take this next caller. Caller, where are you from?
Caller: I’m from right here in town. I was curious to know - I heard you talking about the vitamin D and the thyroid and the magnesium. I was just wondering if that would have anything to do with what’s called “restless leg syndrome”?
HD2: Yes, that’s a magnesium deficiency. Dr Peat, how would you explain restless leg syndrome?
RP: There has been quite a lot of research about it and, for example, they noticed that people taking SSRI antidepressants tended to have episodes of restless legs and so they saw that Nitric Oxide (NO) and serotonin were involved in producing it. Those are produced largely from the intestine. The most intense problem of both serotonin and NO production is from an irritated intestine and hypothyroid people overproduce both NO and serotonin typically and have sluggish digestive systems and often have a tendency to generalized inflammation. And the serotonin seems to be specifically what pushes those motor nerves that cause the leg jumpiness.
HD1: Does that help you out or explain things to you, Caller?
Caller: Yeah. So it’s not an adrenalin thing that makes the legs jump - it’s serotonin?
RP: All of the inflammatory stress things tend to go together.
HD2: So, would you recommend aspirin for restless leg syndrome?
RP: Yep, pregnenolone, aspirin, and avoiding irritating foods, especially legumes and raw green salads. Those are very irritating.
HD2: Those are things that increase the bowel production of serotonin.
RP: Yeah.
HD2: Beans and raw vegetables?
Caller: That’s interesting; cause we just switched to trying to eat better and we had gone to eating more of both of those!
HD2: Had you noticed that your restless leg syndrome had increased?
Caller: It’s a female, and my partner, who experiences this and is becoming very extreme and so that may very well be just from the diet, huh? And she has a vitamin D deficiency and she was told to take vitamin d and magnesium.
HD2: Do you know what her vitamin D level was and how much she is taking? Caller: I don't know exactly in measurement, but it was very low.
HD1: Well, most drop forms of vitamin D now are 2,000 IU a drop and if she has low vitamin D it’s probably below 20, maybe right around 20, which is very low, and they’ve raised the reference limit now for vitamin D to about 45 - so if you are supplementing with a 2,000 IU per day drop product, she should really be loading up with 6-8 drops a day for about 4 or 5 days and then getting around 4,000 to 6,000 IU and then re-measuring her vitamin D levels.
HD2: After about 2 months.
HD1: So, Dr Peat said that bowel irritation/inflammation increases serotonin production and that serotonin production with NO which we have another question for Dr Peat about NO. Both those two compounds there can be predisposing someone to restless leg syndrome. Anyway, thanks for your call.
HD1: So, Dr Peat I saw, today just in fact - and I was thinking about it myself and started looking at a couple of websites that do blood testing etc. and I couldn’t see any NO blood testing tests done - but I did see salivary tests for – they were salivary nitrite strips to assess the potential NO production in the body. I know it will be formed from nitrate or nitrite. This is the funny thing, this site actually was letting you know how you could increase NO more by eating various foods which I wanted to question you about also - so I know some of the greens here that are promoting the NO production are some of the things that we are actually promoting as being beneficial but there’s obviously a reason for that. So how do you feel about testing your salivary nitrate/nitrite level and how predictive or pre-emptive that would be of NO production systemically?
RP: A recent article just a couple of weeks ago came out suggesting measuring the NO or its products in the body as a way of diagnosing hypothyroidism because they are so closely connected, but I would guess that the urine might be better than the saliva because for other hormone testing, for example, just thinking of food or being anxious or whatever can really change the composition of your saliva.
HD1: OK, so because that changes so quickly, your saying, that it is more relative to test something that’s there and it’s stored and probably more representative of a couple of hours of physiology?
RP: Yeah. I think that the urine will give you a good picture of your level of stress.
HD2: You wouldn’t want to test it after eating spinach either with your saliva.
HD1: Here’s the other thing – this was my other question - this website was touting NO as being beneficial and actually spinach was a very good producer of nitrate, and how spinach will increase your NO - and they were touting that - and I know and I want to ask you here just to be realistic and be real for folks - I know we mentioned greens, purporting greens, and boiled greens and drinking the juice as very beneficial and I know that you do say kale can have a thyroid suppressant effect - so not to use to much kale - but spinach I think has been one of those greens that has been portrayed as being relatively healthy - so what do you think about spinach?
RP: If they are organically grown without intense nitrate fertilization and if it’s well cooked, I think spinach is good food.
HD1: Let’s take this next caller. Caller, where are you from?
HD1: You’re on the air, where are you calling from?
Caller: Hi, I’m from Shelter Cove. My question is for my daughter actually. She wants to take testosterone and I’m wondering what Dr Peat’s take is on it and if he has any experience on that and how she can keep herself healthy?
HD1: How old is she and what is the indication for taking the testosterone? Caller: Well, she is transgender and wants to be more male and she is 16.
RP: Wanting to masculinize?
Caller: Yes.
RP: I think that’s safe but it should be backed up with pregnenonlone and some progesterone to keep things in balance because the tendency is, if you are under stress of any sort, for the testosterone to turn to oestrogen and the pregnenolone and progesterone will limit that conversion.
Caller: OK.
HD1: Do you have access to those? Both of those can be obtained, so progesterone and pregnenolone, typically for a female anyway they would normally be producing them and I don't know the exact details of the case and how the transgender nature of this subject is either affected her adversely or positively and so in terms of their exposure to their own natural progesterone being female and/or supplementing with pregnenolone, then that would offset the potentially negative effects that may occur with using testosterone in a female.
HD2: Cause it could convert to oestrogen and become dangerously out of balance. RP: And watching thyroid function.
Caller: OK. Thanks for your help.
HD1: I don't even know if we have enough time to ask another question without running out of time, but I’ll try here. And I think we will definitely open this up for the next month if you are available cause we hardly got any questions asked cause we had so many callers and that’s a good thing. I wanted to ask you again with the female issue and oestrogen and inflammation and cancers etc., pretty obvious as definite realities here. In terms of the effects of iodine uptake by thyroid cells, and the inhibitory effects oestrogen has on that, in a female, again would you be just typically wanting to lower oestrogen burden by offsetting that with progesterone and pregnenolone and/or thyroid?
RP: Yeah, thyroid and good adequate nutrition. All the vitamins and minerals are involved in controlling and keeping oestrogen under the safe limit. And when you inhibit the formation of thyroid hormone, either with an iodine deficiency or an oestrogen excess, the TSH fails to make the thyroxin and T3 and so it keeps stimulating not only the thyroid gland, making it grow and get bigger or nodules to form, but it has a related effect on every tissue to some extent - especially the ovaries. Polycystic ovarian syndrome (PCOS) is associated with low thyroid and especially high TSH. TSH drives inflammation so that the so- called autoimmune conditions associated with high oestrogen - women are far more susceptible to all types of autoimmune diseases than males - and that's largely because of the high TSH exposure driving things like tumor necrosis factor and the various cytokines, and interleukins and prostaglandins that are activated.
HD1: Excellent. I don’t want to cut you short Dr Peat and I really appreciate your knowledge, as do I know all the people that are tuned in and taken the time to listen and to call from all over. A really good show from people all over the country and I really appreciate people calling. Thanks very much, Dr Peat.
www.raypeat.com
_______________________