cjm
Member
Full text and link below. Further down, some comments.
"TWO CASES OF FATAL SALICYLATE POISONING AFTER TOPICAL APPLICATION OF AN ANTIFUNGAL SOLUTION
C. PAUL LINDSEY, M.B., B.S. (District Medical Officer)
Bougainville, T.P.N.G.
Two cases of fatal salicylate poisoning are reported. Whilst aspirin has become an increasingly unfashionable poison amongst adults [edit: lol], and the clinical effects of salicylism are less commonly seen than in the past, fatal salicylate poisoning still occurs, as these unusual iatrogenic cases illustrate.
CLINICAL RECORD
On April 29, 1967, two brothers, K. and W., Sepik labourers working on a coastal plantation in Bougainville, were painted over 50% of their total body areas respectively with a proprietary "grilli" lotion. This was done twice that day. Grilli, or tinea imbricata, is an extremely common cutaneous fungous infection (caused by Trichophyton concentricum) within the Territory of Papua and New Guinea. The lotion with which they were painted was found by Dr. R. A. Cooke to be an alcoholic solution of salicylic acid (20.7%), iodine (3.2%) and potassium iodide (2.8%). Within six hours, both brothers became unwell, and were given the day off. Both were slightly mentally confused, W. more so than his brother.
That evening, W. vomited and became unconscious and febrile, and was noted to be breathing very rapidly. His brother, K., also developed rapid respiration, and became extremely restless, walking with incoordinate gait and talking and behaving wildly. Eventually he had to be restrained. The next morning he was found unconscious. Both were placed on a boat at 11 a.m., and arrived at Kieta Hospital at 4 p.m. W. was dead on arrival.
On examination, K. was deeply comatose, with a temperature of 42° C. The skin was blistered over both shoulders. His blood pressure was 90/40 mm. Hg, and his pulse rate was 160 per minute. His muscle tone was flaccid and no response to stimuli could be elicited. His respirations numbered 35 per minute, his breathing being shallow but regular. Examination of a blood film for malaria parasites showed none present. Cooling measures were immediately initiated, and vigorous resuscitation was commenced. Despite this, the patient's temperature remained elevated, his respirations became gasping and irregular, and he died at 4.45 p.m. on April 30.
A post-mortem examination performed on both patients revealed nothing abnormal that would account for their deaths, and the findings on microscopic examination were normal also. The solution with which the brothers were painted was analysed.
Since the clinical signs and symptoms were consistent with salicylate poisoning, and since the proprietary "grilli" lotion contained a concentration of salicylic acid twice that recommended by the Public Health Department in the Territory, the cause of the deaths was diagnosed as salicylate poisoning, which diagnosis was accepted by the coroner's court.
DISCUSSION
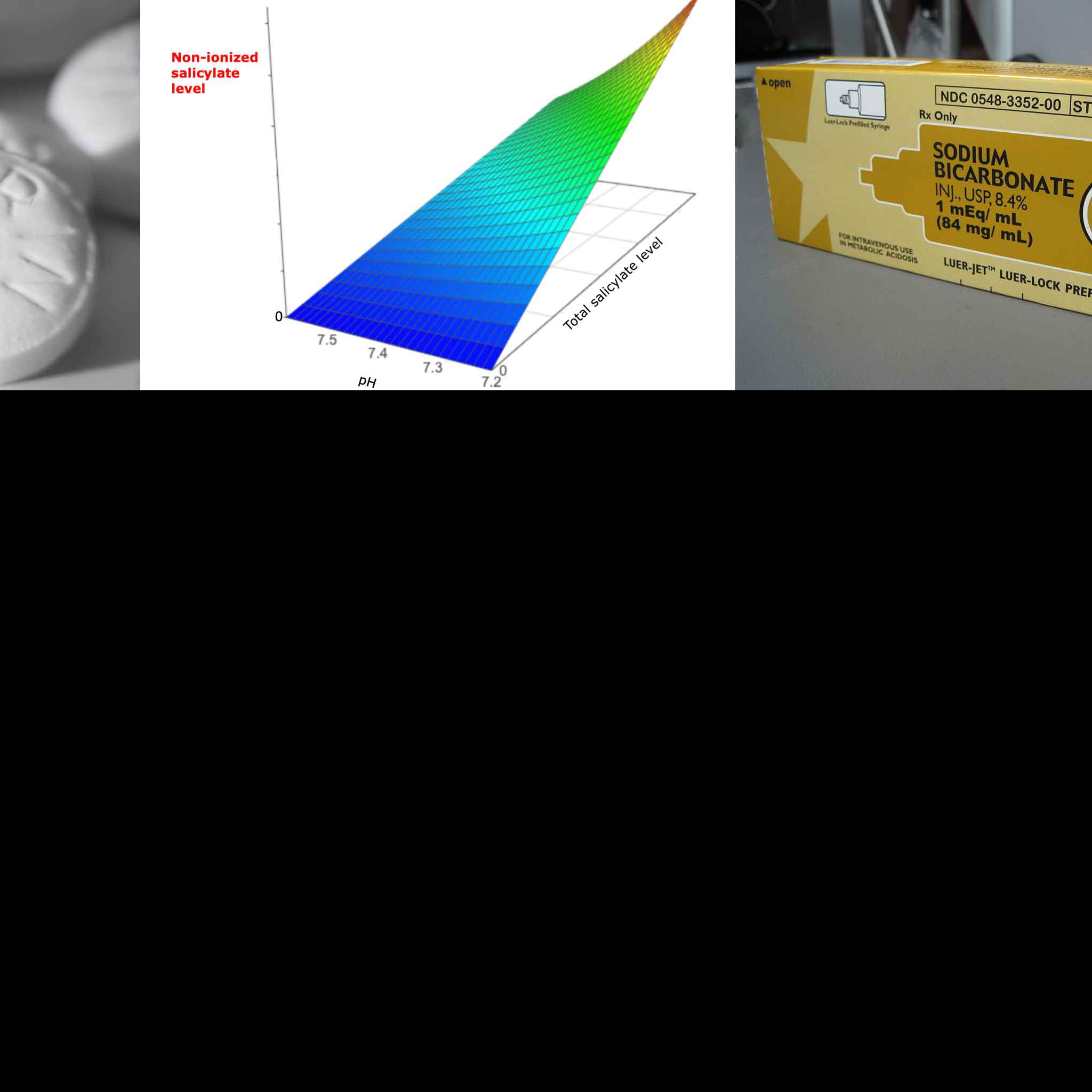
Salicylates are absorbed readily through the skin, and toxic effects will be seen when the blood level reaches 30 mg. per 100 ml. The salicylate acts directly on the respiratory centres, producing hyperpnoea and then respiratory alkalosis. Subsequent vomiting with loss of base, disturbed renal function and derangement of carbohydrate metabolism eventually lead to a decompensated acidosis.
Clinical signs of acute salicylic toxicity include hyperpnoea, vomiting, sweating, hyperpyrexia, dehydration, irritability, delirium, incoordination, restlessness, coma and respiratory failure. All these signs were seen here. Also, signs of acute salicylism are tinnitus, abdominal pain, cyanosis, ecchymoses and ureemla (Dreisbach, 1963).
The recommended formula of the treatment of tinea imbricata is as follows: salicylic acid, 10%; malachite green, 0,1%; and alcohol, 70%; to make 100 parts of sipoma paint (Public Health Department Handbook, 1962). "The Extra Pharmacopreia (Martindale)" (Council of the Pharmaceutical Society of Great Britain, 1958) suggests a strength of salicylic acid from 2% to 10%. Never more than one-fifth of the total body area should be painted at one time or within 24 hours; nor is it wise to prolong a course of treatment for more than, say, five days. Symptoms of acute salicylate poisoning have been reported ("Martindale", 1958) in children after prolonged application of salicylic acid ointment to large areas of the body surface. Evidently rapid absorption occurs when alcoholic solutions are applied.
The indiscriminate and untutored application of grilli lotions of uncertain ingredients effects very little good, since the patient usually returns to don his dirty clothes, and even after a supervised treatment in hospital, recurrence of the fungous infection is the rule. The dangers of treatment are commonly forgotten, until the public's attention is drawn to them by fatalities such as these.
SUMMARY
Two cases of death from salicylate poisoning due to topical application of 20.7% salicylic acid in alcohol are described."
~~
~~
This is what the two brothers were trying to treat:
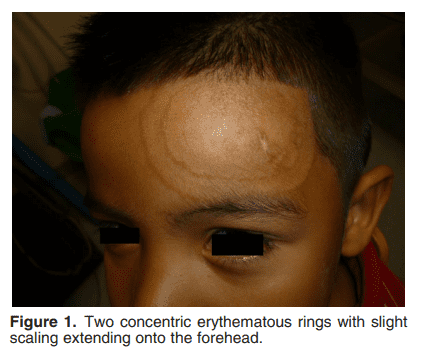
Tinea Imbricata as a Clue to Occult Immunodeficiency (Jimenez et al., 2014)
Grilli lotion is similar to an old formulation called Whitfield's Ointment that was first developed in 1907. It can be used to treat grilli, or tinea imbricata.
“The Whitfield’s ointment (10 % benzoic acid and 10 % salicylic acid in vaseline and lanoline) is helpful to remove squamous and hyperkeratotic lesions.” Tinea Imbricata in an Italian Child and Review of the Literature (Veraldi et al., 2015)
Product link: Bunny's Jamaican Whitfield's Ointment 28g, Double Strength, Treatment for Fungus Infection of The Skin
Fungal infection can lead to organ failure:
"Fungi usually enter the human body through the respiratory tract and are then disseminated to the central nervous system (CNS) via the blood. However, fungi (including Exophiala dermatitidis and E. rostratum) can directly infect the CNS or bone marrow of even immunocompetent individuals in cases of surgery, trauma, intravenous drug use, or exposure to contaminated medical supplies. Fungi can also be spread from adjacent tissues (sinus structures, mastoids, or eyelids) to the CNS." Multiple organ dysfunction caused by severe fungal infection: report of one case and a literature review (Xiao et al., 2019)
Benzoic acid, as in Whitfield's Ointment, is a natural defense against fungal infection (and a growth/yield (read: health) promoter):
“Tomato early blight, caused by Alternaria solani, is a destructive foliar fungal disease. Herein, the potential defensive roles of benzoic acid (BA) and two of its hydroxylated derivatives, ρ-hydroxybenzoic acid (HBA), and protocatechuic acid (PCA) against A. solani were investigated. All tested compounds showed strong dose-dependent fungistatic activity against A. solani and significantly reduced the disease development. Benzoic acid, and its hydroxylated derivatives, enhanced vegetative growth and yield traits. Moreover, BA and its derivatives induce the activation of enzymatic (POX, PPO, CAT, SlAPXs, and SlSODs) and non-enzymatic (phenolics, flavonoids, and carotenoids) antioxidant defense machinery to maintain reactive oxygen species (ROS) homeostasis within infected leaves.” Benzoic Acid and Its Hydroxylated Derivatives Suppress Early Blight of Tomato (Alternaria solani) via the Induction of Salicylic Acid Biosynthesis and Enzymatic and Nonenzymatic Antioxidant Defense Machinery (Nehela et al., 2021).
“Whitfield ointment (WO) is an antiseptic ointment that was widely used in the past to treat topical fungal infections but seldom used currently because of the availability of new therapies. The reasons for the underutilization of the Whitfield ointment could be its tendency to irritate the skin (especially in flexures and face) and being less targeted to dermatophytes than the newer therapies. Its efficacy has been shown to be equal to other topical antifungal in several studies....It combines the fungistatic action of benzoic acid with the keratolytic action of salicylic acid. The original formula contains 6% benzoic acid and 3% salicylic acid and World Health Organization (WHO) suggested a modified Whitfield ointment (MWO) with 5% benzoic acid and 5% salicylic acid for tropical countries.... It is economical and can be manufactured locally.” Treatment of difficult-to-treat-dermatophytosis: results of a randomized, double-blind, placebo-controlled study (Fonseka et al, 2021)
~
~
My next post may or may not be about the often forgotten primary action of salicylic acid, keratolysis, or peeling, as well as the vast benefits of its metabolite, benzoic acid.
"TWO CASES OF FATAL SALICYLATE POISONING AFTER TOPICAL APPLICATION OF AN ANTIFUNGAL SOLUTION
C. PAUL LINDSEY, M.B., B.S. (District Medical Officer)
Bougainville, T.P.N.G.
Two cases of fatal salicylate poisoning are reported. Whilst aspirin has become an increasingly unfashionable poison amongst adults [edit: lol], and the clinical effects of salicylism are less commonly seen than in the past, fatal salicylate poisoning still occurs, as these unusual iatrogenic cases illustrate.
CLINICAL RECORD
On April 29, 1967, two brothers, K. and W., Sepik labourers working on a coastal plantation in Bougainville, were painted over 50% of their total body areas respectively with a proprietary "grilli" lotion. This was done twice that day. Grilli, or tinea imbricata, is an extremely common cutaneous fungous infection (caused by Trichophyton concentricum) within the Territory of Papua and New Guinea. The lotion with which they were painted was found by Dr. R. A. Cooke to be an alcoholic solution of salicylic acid (20.7%), iodine (3.2%) and potassium iodide (2.8%). Within six hours, both brothers became unwell, and were given the day off. Both were slightly mentally confused, W. more so than his brother.
That evening, W. vomited and became unconscious and febrile, and was noted to be breathing very rapidly. His brother, K., also developed rapid respiration, and became extremely restless, walking with incoordinate gait and talking and behaving wildly. Eventually he had to be restrained. The next morning he was found unconscious. Both were placed on a boat at 11 a.m., and arrived at Kieta Hospital at 4 p.m. W. was dead on arrival.
On examination, K. was deeply comatose, with a temperature of 42° C. The skin was blistered over both shoulders. His blood pressure was 90/40 mm. Hg, and his pulse rate was 160 per minute. His muscle tone was flaccid and no response to stimuli could be elicited. His respirations numbered 35 per minute, his breathing being shallow but regular. Examination of a blood film for malaria parasites showed none present. Cooling measures were immediately initiated, and vigorous resuscitation was commenced. Despite this, the patient's temperature remained elevated, his respirations became gasping and irregular, and he died at 4.45 p.m. on April 30.
A post-mortem examination performed on both patients revealed nothing abnormal that would account for their deaths, and the findings on microscopic examination were normal also. The solution with which the brothers were painted was analysed.
Since the clinical signs and symptoms were consistent with salicylate poisoning, and since the proprietary "grilli" lotion contained a concentration of salicylic acid twice that recommended by the Public Health Department in the Territory, the cause of the deaths was diagnosed as salicylate poisoning, which diagnosis was accepted by the coroner's court.
DISCUSSION
Salicylates are absorbed readily through the skin, and toxic effects will be seen when the blood level reaches 30 mg. per 100 ml. The salicylate acts directly on the respiratory centres, producing hyperpnoea and then respiratory alkalosis. Subsequent vomiting with loss of base, disturbed renal function and derangement of carbohydrate metabolism eventually lead to a decompensated acidosis.
Clinical signs of acute salicylic toxicity include hyperpnoea, vomiting, sweating, hyperpyrexia, dehydration, irritability, delirium, incoordination, restlessness, coma and respiratory failure. All these signs were seen here. Also, signs of acute salicylism are tinnitus, abdominal pain, cyanosis, ecchymoses and ureemla (Dreisbach, 1963).
The recommended formula of the treatment of tinea imbricata is as follows: salicylic acid, 10%; malachite green, 0,1%; and alcohol, 70%; to make 100 parts of sipoma paint (Public Health Department Handbook, 1962). "The Extra Pharmacopreia (Martindale)" (Council of the Pharmaceutical Society of Great Britain, 1958) suggests a strength of salicylic acid from 2% to 10%. Never more than one-fifth of the total body area should be painted at one time or within 24 hours; nor is it wise to prolong a course of treatment for more than, say, five days. Symptoms of acute salicylate poisoning have been reported ("Martindale", 1958) in children after prolonged application of salicylic acid ointment to large areas of the body surface. Evidently rapid absorption occurs when alcoholic solutions are applied.
The indiscriminate and untutored application of grilli lotions of uncertain ingredients effects very little good, since the patient usually returns to don his dirty clothes, and even after a supervised treatment in hospital, recurrence of the fungous infection is the rule. The dangers of treatment are commonly forgotten, until the public's attention is drawn to them by fatalities such as these.
SUMMARY
Two cases of death from salicylate poisoning due to topical application of 20.7% salicylic acid in alcohol are described."
~~
~~
This is what the two brothers were trying to treat:
Tinea Imbricata as a Clue to Occult Immunodeficiency (Jimenez et al., 2014)
Grilli lotion is similar to an old formulation called Whitfield's Ointment that was first developed in 1907. It can be used to treat grilli, or tinea imbricata.
“The Whitfield’s ointment (10 % benzoic acid and 10 % salicylic acid in vaseline and lanoline) is helpful to remove squamous and hyperkeratotic lesions.” Tinea Imbricata in an Italian Child and Review of the Literature (Veraldi et al., 2015)
Product link: Bunny's Jamaican Whitfield's Ointment 28g, Double Strength, Treatment for Fungus Infection of The Skin
Fungal infection can lead to organ failure:
"Fungi usually enter the human body through the respiratory tract and are then disseminated to the central nervous system (CNS) via the blood. However, fungi (including Exophiala dermatitidis and E. rostratum) can directly infect the CNS or bone marrow of even immunocompetent individuals in cases of surgery, trauma, intravenous drug use, or exposure to contaminated medical supplies. Fungi can also be spread from adjacent tissues (sinus structures, mastoids, or eyelids) to the CNS." Multiple organ dysfunction caused by severe fungal infection: report of one case and a literature review (Xiao et al., 2019)
Benzoic acid, as in Whitfield's Ointment, is a natural defense against fungal infection (and a growth/yield (read: health) promoter):
“Tomato early blight, caused by Alternaria solani, is a destructive foliar fungal disease. Herein, the potential defensive roles of benzoic acid (BA) and two of its hydroxylated derivatives, ρ-hydroxybenzoic acid (HBA), and protocatechuic acid (PCA) against A. solani were investigated. All tested compounds showed strong dose-dependent fungistatic activity against A. solani and significantly reduced the disease development. Benzoic acid, and its hydroxylated derivatives, enhanced vegetative growth and yield traits. Moreover, BA and its derivatives induce the activation of enzymatic (POX, PPO, CAT, SlAPXs, and SlSODs) and non-enzymatic (phenolics, flavonoids, and carotenoids) antioxidant defense machinery to maintain reactive oxygen species (ROS) homeostasis within infected leaves.” Benzoic Acid and Its Hydroxylated Derivatives Suppress Early Blight of Tomato (Alternaria solani) via the Induction of Salicylic Acid Biosynthesis and Enzymatic and Nonenzymatic Antioxidant Defense Machinery (Nehela et al., 2021).
“Whitfield ointment (WO) is an antiseptic ointment that was widely used in the past to treat topical fungal infections but seldom used currently because of the availability of new therapies. The reasons for the underutilization of the Whitfield ointment could be its tendency to irritate the skin (especially in flexures and face) and being less targeted to dermatophytes than the newer therapies. Its efficacy has been shown to be equal to other topical antifungal in several studies....It combines the fungistatic action of benzoic acid with the keratolytic action of salicylic acid. The original formula contains 6% benzoic acid and 3% salicylic acid and World Health Organization (WHO) suggested a modified Whitfield ointment (MWO) with 5% benzoic acid and 5% salicylic acid for tropical countries.... It is economical and can be manufactured locally.” Treatment of difficult-to-treat-dermatophytosis: results of a randomized, double-blind, placebo-controlled study (Fonseka et al, 2021)
~
~
My next post may or may not be about the often forgotten primary action of salicylic acid, keratolysis, or peeling, as well as the vast benefits of its metabolite, benzoic acid.
Last edited: